The story behind ATLS
Origin of ATLS
Why ATLS exists
ATLS was created to standardise the first hour of trauma care — so any clinician, in any hospital, can deliver a safe, structured approach to immediately life-threatening problems.
Key timeline
- February 1976: Dr James K. Styner crashed his plane in rural Nebraska. Noticing a worrying lack of emergency trauma training at the local hospital, he highlighted major variability and gaps in trauma care.
- 1978: The first prototype ATLS course was delivered locally, turning the "what should we do first?" problem into a teachable system.
- 1980: The American College of Surgeons (ACS) adopted and began wider dissemination of ATLS.
Take-home: ATLS is a shared language — prioritise threats, intervene early, reassess repeatedly.
🎯 Learning objectives
By the end of this module, you should be able to:
- Explain the purpose and philosophy of ATLS.
- Describe the primary survey using the ABCDE approach.
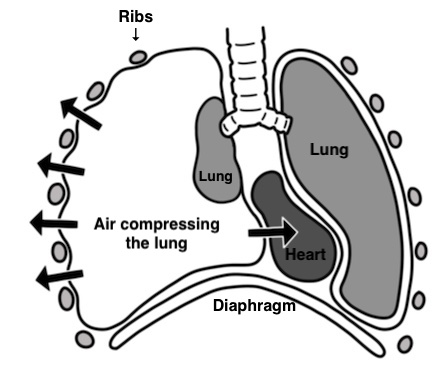
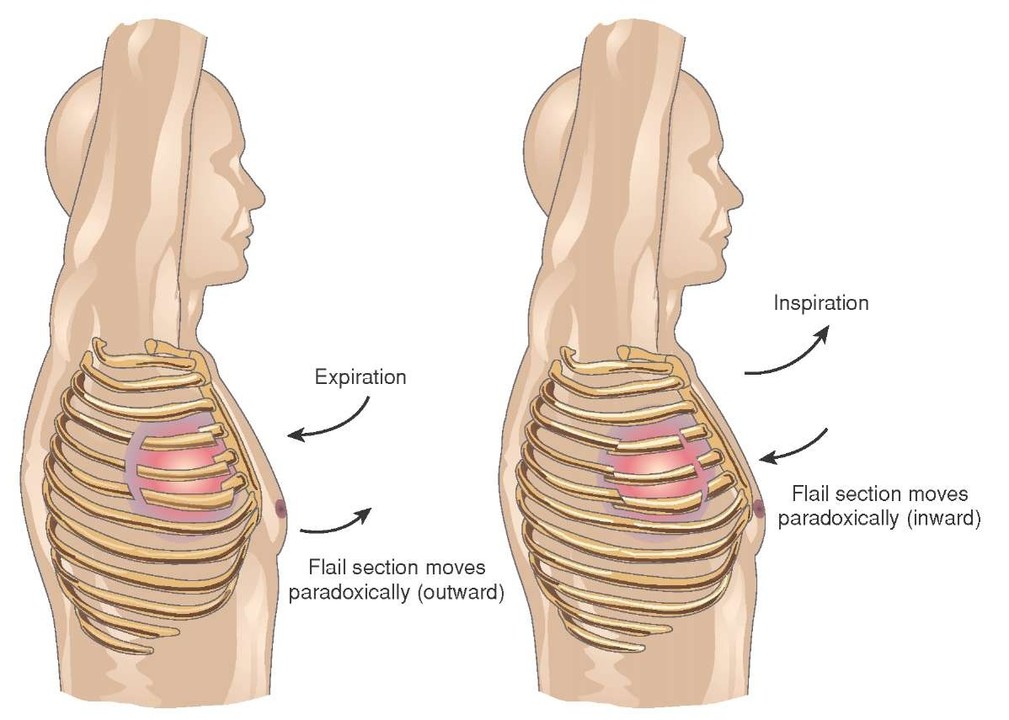
- Recognise life-threatening injuries.
- Understand the difference between primary and secondary survey.
- Appreciate the importance of team roles and communication.
- Apply ATLS principles to a trauma case.
⚠️ This module is not a substitute for the formal ATLS course delivered by the Royal College of Surgeons of England. It is designed as a brief overview and supplementary learning resource.