Necrotising Fasciitis
A practical interactive module for UK healthcare professionals, covering the recognition, pathophysiology, classification, time-critical resuscitation, and emergency surgical management of necrotising fasciitis — a rapidly progressive, life-threatening soft tissue infection.
Time-critical: Necrotising fasciitis is a surgical emergency. Delay to surgical debridement beyond 6 hours is associated with significantly increased mortality.
What is necrotising fasciitis?
Necrotising fasciitis is a rare but rapidly progressive skin and soft tissue infection characterised by invasion of the deep fascial layers, causing diffuse microvascular occlusion and necrosis. It spreads along fascial planes, often far beyond the visible skin changes, and carries a high mortality if not recognised and treated promptly.
Absence of pus
A notable absence of frank pus. Instead, a thin, foul, greyish “dishwater” exudate is characteristic at exploration.
Widespread necrosis
Destruction extends from dermis to deep muscle and tendon, accompanied by severe, disproportionate pain.
Rapid progression
Progresses rapidly — potentially to septic shock and death within hours of presentation.
Often trivial injury
Arises from minor skin injuries, muscle strains, insect bites, or post-operative obstetric/gynaecological procedures.
NF occurs in both immunocompromised and previously well, immunocompetent hosts. The approach to diagnosis and treatment is the same in either group.
How tissue is destroyed
A breach in the skin or mucosa allows organisms to enter the soft tissues. A deep tissue injury combined with bacteraemia can seed infection. As part of the repair response, inflammatory mediators draw organisms to the site of injury. The organisms release exotoxins that damage local tissues and occlude capillaries, disrupting the vascular supply. Venous occlusion and microvascular thrombosis cause progressive ischaemia and necrosis, producing the erythema, swelling, and ecchymosis/bullae seen clinically.

From “hospital gangrene” to a modern misnomer
An army surgeon is first credited with describing the condition, then known as “hospital gangrene.” Its incidence has risen over recent decades. In the 1990s the media coined the term “flesh-eating bacteria” — a misnomer, since the bacteria do not eat tissue but destroy it through toxin-mediated ischaemia. There is also a common misconception that NF only affects high-risk patients.

Susceptible host
Diabetes mellitus, immunocompromise, excessive alcohol intake, obesity, the sedentary/elderly, and malnourishment.
Portal of entry
IV drug use, hypodermic therapeutic injections, insect bites, skin abrasions, ulcers/skin conditions, and abdominal or perineal surgery.
Why classify?
NF is classified microbiologically into four types. While the type guides antibiotic choice and identifies typical host groups, all types require urgent surgical evaluation. Delay greater than 6 hours is associated with increased mortality regardless of type.
Polymicrobial. The most common type. Often elderly, diabetic patients, pressure ulcers, and post-operative abdominal or perineal infections.
Group A beta-haemolytic Streptococcus (and Staphylococcus aureus). Can affect all ages, often with no underlying disease.
Marine-related organisms and Clostridia infections, which can lead to gas gangrene.
Fungal. Predominantly affects immunocompromised patients.
Type II — the one not to miss in the well patient
- Affects all ages, often with no underlying disease
- No portal of entry found in around 50% of cases
- Bacteraemia is common — frequently presents with rigors
- 30–70% mortality; patients may die within 12 hours without surgical intervention
- Exotoxin-mediated toxic shock syndrome
- More than 25% require amputation
Extremities (~75%)
The limbs are by far the most frequent site of necrotising soft tissue infection.
Neck
Includes Ludwig’s angina and Lemierre’s syndrome.
Fournier’s gangrene
Necrotising infection of the perineum and external genitalia.
Abdominal wall
May involve the abdominal wall, with colonic or peritoneal sources.
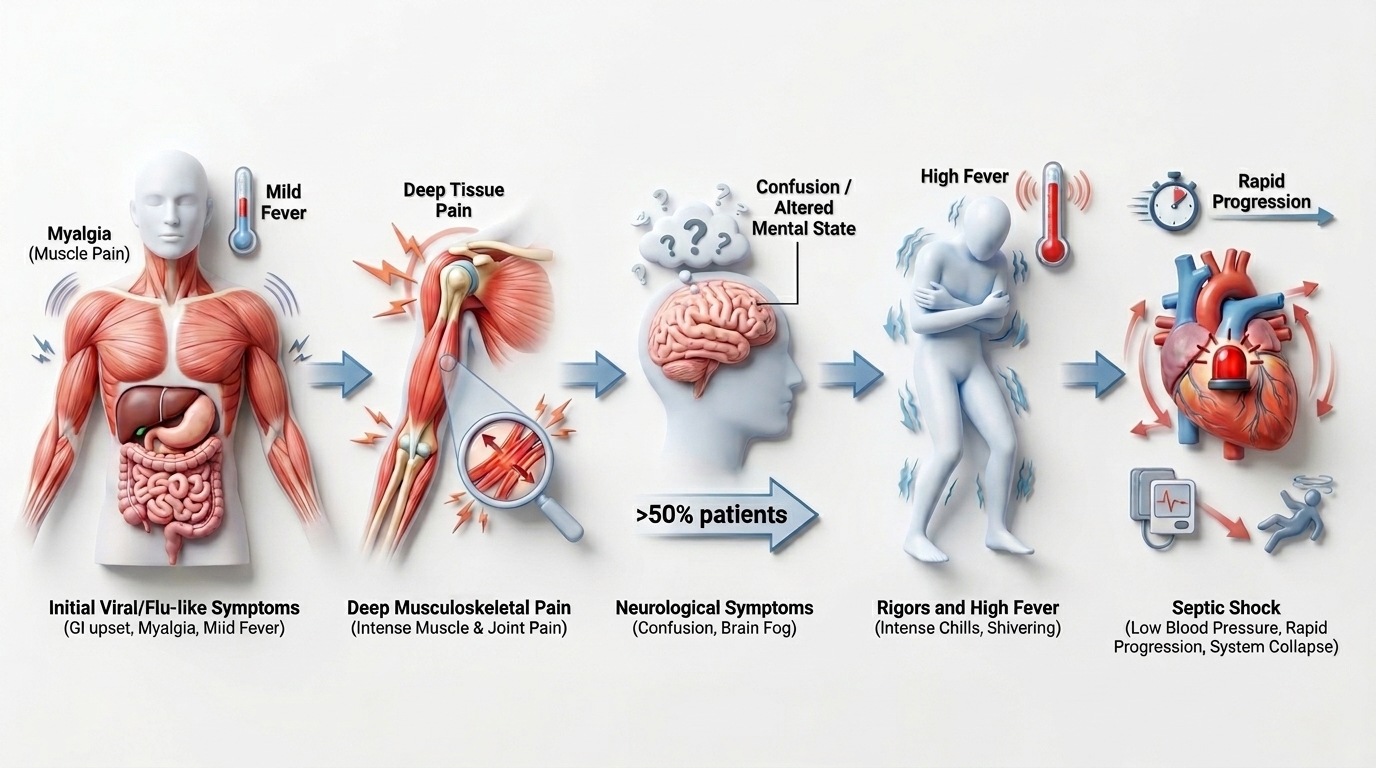
Systemic features
Initial viral/flu-like symptoms (myalgia, GI upset); severe pain deep in muscle/joint; confusion or altered mental state in >50% of patients; rigors and high fever; rapid progression to septic shock.
Local features
Pain out of proportion to examination findings; erythema, tenderness, and warmth; rapid-onset skin rash and blisters; bullae, crepitus, and anaesthesia. The site of entry is often not found.
Activity complete
| Feature | Cellulitis | Necrotising fasciitis |
|---|---|---|
| Threat to life | Not usually life-threatening | Life-threatening |
| Progression | Slow, indolent | Rapidly progressive |
| Pain | Pain not severe | Severe pain, often beyond the visibly involved area |
| Systemic state | No signs of systemic shock | Septic |
| Antibiotic response | Responds to broad-spectrum antibiotics | Does not respond to antibiotics alone |
| Margins | Distinct margins | Indistinct margins |
| Skin changes | — | Bullae formation, skin sloughing, tissue necrosis |
Cellulitis can progress to necrotising fasciitis. Reassess any “cellulitis” that deteriorates rapidly, fails to respond, or develops disproportionate pain.
Features that should raise immediate concern
- Pain out of all proportion to clinical findings
- Altered mental state
- Erythema progressing rapidly along the limb
- Fluctuance
- Haemorrhagic bullae
- Skin necrosis
Sepsis with organ hypoperfusion — septic shock
- Hypotension < 90 mmHg systolic
- Hypoxia
- Lactate > 2
- AKI / raised creatinine
- DIC / thrombocytopenia
- Liver dysfunction
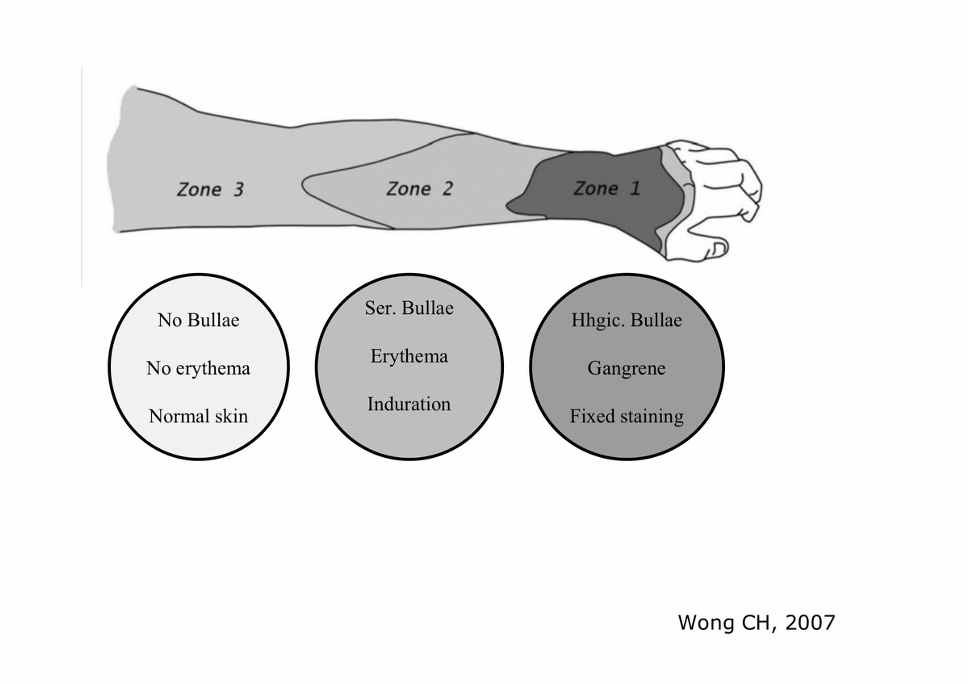
Erythema & pain
Tenderness beyond the apparent margin, warmth, and erythema, with pain out of proportion to the visible findings.
Blistering
Blister and bulla formation, with skin changes evolving over hours.
Haemorrhagic bullae, necrosis & crepitus
Haemorrhagic bullae, skin necrosis/sloughing, anaesthesia of the overlying skin, and crepitus are late signs — surgery should not wait for them.

Erythema & pain

Blistering

Haemorrhagic bullae, necrosis & crepitus
NF is primarily a clinical and surgical diagnosis. If clinical suspicion is high, do not delay surgical exploration for imaging or scores.
History & examination
Take a focused history and examine the limb. Mark the area of erythema and record the date and time to track rapid progression.
Sepsis Six
Initiate the Sepsis Six promptly — oxygen, blood cultures, IV antibiotics, IV fluids, lactate, and urine output monitoring.
Bloods & imaging
- Labs: CRP, procalcitonin (PCT), and group & save (G&S), alongside FBC, U&Es, lactate, and clotting
- Imaging: reserve for cases of lower clinical suspicion — it must not delay theatre when suspicion is high
- Point-of-care ultrasound may show a thickened fascial layer and fluid tracking along fascial planes
Bedside / intra-operative finger test
Under local or general anaesthesia, a small incision is made down to the deep fascia and a gloved finger is used to probe along the fascial plane. Findings suggestive of NF include:
- “Dishwater” fluid
- Lack of bleeding
- Greyish necrotic tissue
- Tissues that peel off the fascia with minimal resistance
Viewer discretion is advised. The following video contains graphic clinical and surgical footage of necrotising fasciitis.

Laboratory Risk Indicator for Necrotising Fasciitis (LRINEC)
The LRINEC score combines routine laboratory values to stratify the risk of NF. It is an adjunct only and does not replace clinical judgement.
| Parameter | Value | Points |
|---|---|---|
| CRP (mg/L) | < 150 / ≥ 150 | 0 / 4 |
| White cell count (×10&sup9;/L) | < 15 / 15–25 / > 25 | 0 / 1 / 2 |
| Haemoglobin (g/dL) | > 13.5 / 11–13.5 / < 11 | 0 / 1 / 2 |
| Sodium (mmol/L) | ≥ 135 / < 135 | 0 / 2 |
| Creatinine (µmol/L) | ≤ 141 / > 141 | 0 / 2 |
| Glucose (mmol/L) | ≤ 10 / > 10 | 0 / 1 |
A LRINEC score ≥ 6 is a reasonable cut-off to rule in NF, but a score < 6 does not rule out the diagnosis. There are no prospective trials validating the LRINEC score.
Principles of management
Survival depends on early diagnosis and emergency surgery combined with aggressive resuscitation. This is a multidisciplinary emergency from the outset.
Recognise & escalate
Early diagnosis and emergency surgical referral. Immediate multidisciplinary input — surgeons, intensive care, and microbiology.
Broad-spectrum antibiotics & resuscitation
Commence broad-spectrum antibiotics and aggressive resuscitation, with supportive care in intensive care.
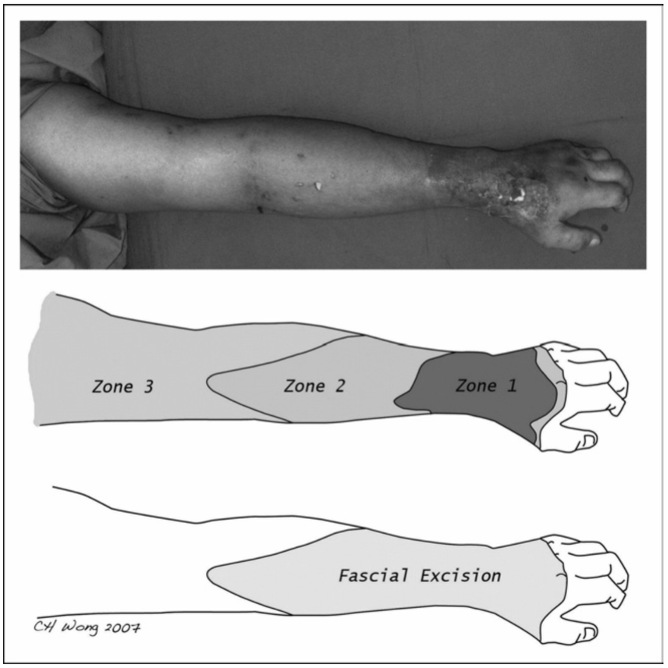
Surgical debridement
Serial debridement until no further necrosis or infection is seen — removing all necrotic skin and tissue, and any tissue of questionable viability.
Constant re-evaluation
At least a 10 mm margin of healthy fascia, with sampling from healthy fascia and planned re-look procedures to confirm source control.
Necrotic tissue
Completely excised, up to the muscle layer.
Infected but salvageable
Meticulously assessed. Fascia must be excised with at least a 10 mm margin of healthy fascia.
Non-infected skin
Left alone. However, any area of skin and subcutaneous tissue that can be easily lifted off the muscle is involved and must be excised.
🩹 Plastic surgery input
Early involvement for soft tissue reconstruction once source control is achieved.
🌀 VAC therapy
Negative-pressure wound therapy to manage large wounds and bridge to definitive cover.
🧑⚕️ Tissue viability
Specialist nursing for complex wound care and dressing strategy.
🦵 Physiotherapy
Rehabilitation, including following amputation where limb salvage is not possible.
⚠️ Why NF is so often missed
- Early diagnosis is notoriously difficult and misdiagnosis is common
- Symptoms mimic other infections — frequently labelled “cellulitis”
- Delay in surgical exploration through failure to recognise the signs and lab findings
- Over-reliance on imaging
- The consequence of delay is loss of limb and loss of life
In one study, NF was initially misdiagnosed 71.4% of the time. Maintain a high index of suspicion.
32M, intravenous drug user
Presents to ED at 06:00h with a 1-day history of a painful left lower leg, with fever and confusion for the last 3–4 hours.
Examination: Temp 39.1°C, erythema and a tender left leg. Mildly confused. BP 85/50, HR 120.
Labs: WCC 15.7, Hb 138, lactate 3.8, creatinine 122, Na 132, CRP 309.

Question 1 — What are your differential diagnoses?
DVT, cellulitis, critical limb ischaemia — and necrotising fasciitis. The combination of disproportionate pain, fever, confusion, hypotension, and a markedly raised CRP/lactate in an IV drug user should raise strong suspicion of NF.
Question 2 — What is the LRINEC score, and how do you interpret it?
CRP 309 (4) + WCC 15.7 (1) + Na 132 (2) = 7 (Hb and creatinine score 0; glucose not given). A score ≥ 6 supports the diagnosis — but remember a low score would not exclude NF, and clinical suspicion already mandates surgical review.
Question 3 — What is your immediate management?
Sepsis Six and aggressive resuscitation, broad-spectrum IV antibiotics, and immediate referral for emergency surgical exploration with intensive care and microbiology input. Mark the erythema with the time. This patient was admitted to ICU and taken to theatre for surgical debridement.
Question 4 — What are the key surgical principles at debridement?
Excise all necrotic and questionable tissue to a margin of at least 10 mm of healthy fascia, sample healthy fascia for microbiology, and plan serial re-look debridements until no further necrosis is seen.
🏆 Module Complete
You have completed the Necrotising Fasciitis module and reviewed the core principles of recognition, pathophysiology, classification, time-critical resuscitation, and emergency surgical management.
Confirmation of completion
Recognition · LRINEC · Emergency debridement